Diffusion Tensor Imaging of the lower leg: Learnings for muscle contracture and cerebral palsy
Diffusion tensor imaging (DTI) is a magnetic resonance imaging (MRI) technique that exploits the movement of water molecules to reveal microscopic details about tissue architecture. DTI is commonly used in brain imaging studies, used to track neural tracts through the brain. The technique is also ideal for investigating the 3D architecture of muscles, as DTI can be used to obtain detailed, quantitative measurements of the anatomy of complex skeletal muscles in living humans. Prof Robert Herbert’s group at NeuRA utilised the 3T MRI located in the UNSW Node of NIF to take a first look at the compartmentalised soleus muscle to provide reference values for further modelling.
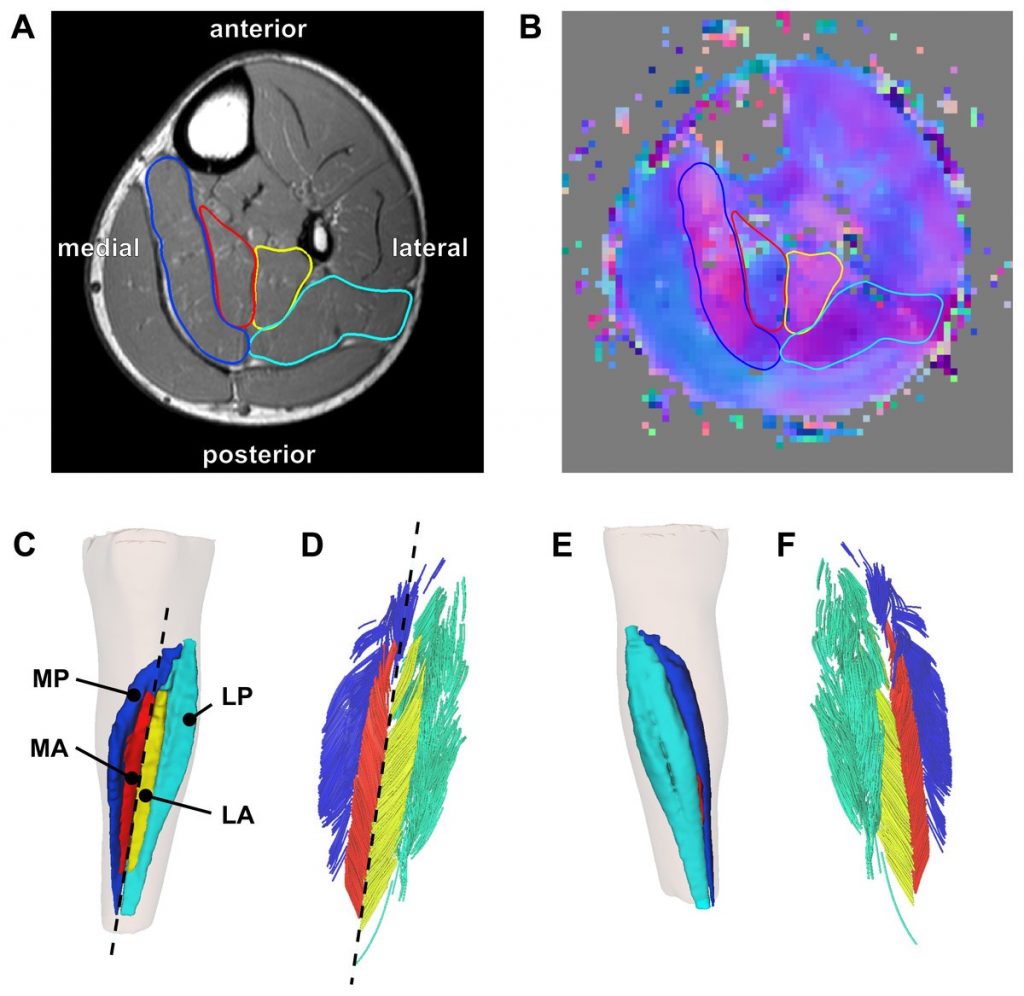
Reconstruction of the architecture of the human soleus muscle using MRI and DTI, taken from ref., showing (A) the MRI slice (midway between ankle and knee) and (B) the corresponding DTI slice taken on a healthy child participant, with (C – F) showing the 3D reconstruction of the surface of all muscle compartments based on the outlines on the anatomical scan.
The human soleus muscle is particularly difficult to study using conventional techniques, such as ultrasound, due to the depth of the anterior and proximal compartments and difficulty in accurate orientation. Hence, DTI is an ideal method to quantify the macroscopic arrangement of muscle fibres of the soleus and help develop comprehensive, quantitative atlases of human muscle architecture.
Prof Herbert’s team have recently used the method to investigate the leg muscles of children with cerebral palsy. Measurements of the medial gastrocnemius muscles were obtained from structural MRI and DTI scans of 20 children with unilateral spastic CP and 20 typically developing children. The study showed that children with unilateral spastic cerebral palsy had reduced range and muscle volume in the calf on the more affected side compared to typically developing children.
The calf plays a vital role in standing and walking, and the differences detected here provide insight into the pathophysiology of muscle contractures and functional impairments in children with cerebral palsy. This knowledge is essential for orthopaedic surgeons and physiotherapists supporting affected children in learning to walk independently.
For further information, please contact NIF Fellow Dr Michael Green.
This story was contributed by NeuRA.


